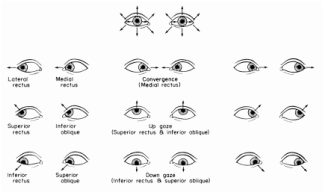
 Today we will be discussing Saccadic Eye Movements. Again I have to tip my hat to Linda Sanet on this one because I love her description of Saccades as "Catching" movements. This to me is a great way to think about saccades, their purpose is to grasp a new object of regard by the fovea. Definition- Sudden voluntary change in fixation from one object of regard to another (definition via the Sanet Volumes). In addition to this sudden voluntary movement there is a certain type of “suppression” (for lack of a better term) or inhibition that takes place in order to avoid awareness of the visual smear during a saccade. :"Static visual stimuli are smeared across the retina during saccades, but in normal conditions this smear is not perceived. Instead, we perceive the visual scene as static and sharp. However, retinal smear is perceived if stimuli are shown only intrasaccadically, but not if the stimulus is additionally shown before a saccade begins, or after the saccade ends" (Campbell & Wurtz, 1978). As to exactly how the filtering process of that smear takes place is not known at this time though researchers think that it is inhibited at the LGN (Lateral Geniculate Body). In this section I also wanted to add a bit of information about the extraocular muscles since it is the firing of these muscles that drive saccadic movement.
For those of you who are interested in learning about the neurology behind eye movements below are links to a video from MIT Open Course Ware that deals with Neural Control of Visually Guided Eye Movements. The videos are lengthy and heavy but worth watching or bookmarking for future reference.  Below is another video about eye movements up close and in slow motion.  Symptoms/Signs when Deficient-
Therapy- In our office one activity we use early on in therapy to train saccadic accuracy is called Hart Chart Saccades and the procedure is as follows: Hart Chart Saccades Purpose: To improve the ability to organize and visually track while maintaining peripheral awareness. Materials: Letter Chart Technique: Level I – Straight Fixations 1.. The patient sits in a relaxed and balanced posture. 2. The Letter Chart is placed at eye level approximately 6’ away. 3. Instruct the patient to read the letters out loud in a rhythmic fashion without moving his head. The patient reads the entire chart proceeding in a left-to-right top-to- bottom fashion. Encourage the patient to maintain peripheral awareness of the whole chart and of other objects in the room. Level II – Line Interiors 1. Starting with the first line of letters, the patient reads out loud the 1st letter, then the last letter, then the 2nd letter, then the next-to-last letter, etc. Each line will be read from the ends to the middle in this fashion. 2. The patient is encouraged to maintain peripheral awareness of the whole chart and of other objects. Variations: 1. Use a metronome set to 60bpm 2..Add distractions such as saying other letters or repeating the alphabet. The assignment that goes along with this topic is as follows:
In the comments below please state your definition of saccades, the signs and symptoms (your own list) when deficient and detailed instruction for one therapy activity you use to address difficulty with saccadic eye movements. Please be as descriptive as possible for the benefit of the group and if you have any links or resources to share please feel free to do so here.
10 Comments
 More Info on Microsaccades More Info on Microsaccades We are going to start slowly with one specific topic and break each one down individually. In this post we will be exploring Fixation. As far as a definition for Fixation my favorite (which I pulled in part from the Sanet Volumes) so far is: Definition- The act of directing the eye toward the object of regard causing, in the normal eye, the image of the object to be centered on the fovea. Fixations are a minute scanning motion not observable by the naked eye made up of high frequency tremors, slow drifts and micro saccades. These mini-movements serve to refresh the image on the retina. One of the main reasons I like this definition is because we often think of fixation as keeping the eyes completely still. This is not the case because if our eyes were completely still the image to which we are attending would disappear as it is not being refreshed on the retina. For anyone interested in more information about microsaccades at the right is a great website link (just click on the picture). An example of an optical illusion that is similar to this fading is called Troxler's Effect. To view this you fixate on the red dot for a few moments and you will see the peripheral blue halo disappear. It will reappear upon changing fixation. 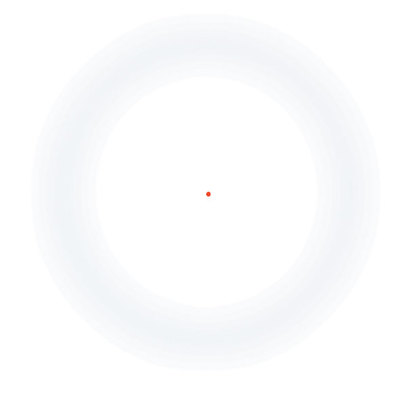 I often think of fixation as being the underlying foundation for eye movements such as saccades and pursuits. If fixation is inadequate all other following eye movements will be inefficient and inaccurate. Since fixation is the foundation the signs/symptoms of deficient fixation would be much the same as with deficient pursuits/saccades Symptoms/Signs when Deficient-
Therapy- In our office one activity we use early on in therapy to train fixation awareness is called Peripheral Penny Snatch and the activity goes as follows; Peripheral Penny Snatch Purpose: To help the patient improve ability to hold their eyes still while maintaining peripheral awareness. Materials: Pennies, plastic cups Technique: 1. Sit on floor facing patient and put a plastic cup in front of you. 2. Instruct patient to sit facing you, keep their eyes on your eyes and don’t look away. 3. Take a penny in each hand and pinch between your index finger and thumb holding them just past your shoulders to start. 4. Ask the patient to take the pennies from your fingertips without looking away from your eyes. Once the patient has successfully taken the penny from the assistant’s fingertip he/she puts it into the cup while maintaining eye contact. If unsuccessful the patient tries again. 5. Give patient feedback appropriate to performance. For example: “Good, you kept your eyes on mine for a little while, and then you peeked. Let’s try it again…” 6. Repeat while holding the penny at a different starting point each time. 7. Since self-awareness is a goal of vision therapy, when possible, ask patient, “How did you do that time?”, etc. Aspects to be emphasized: 1. Awareness of maintaining eye contact (Did they peek?) and peripheral vision. 2. Patient should have good posture, blink and breathe normally. 3. Patient’s ability to grab pennies accurately. The assignment that goes along with this topic is as follows: Hello and welcome to our online study group. This group will be available to any therapist who is currently in the process or will soon be in the process of certifying through COVD. Please follow the directions on the right hand page to join in.
My current plan for the group is to follow the flow of the COVT Candidate Guide. I will post relevant information/articles/book excerpts in these blog type posts. Any questions, answers or comments may be made in the comment section below each post. I will contact anyone who has asked to be included via email when the first post goes up so please email me if you wish to join in, Michelle Beatty, COVT |
VT Study GroupThis group is public and open to anyone that would like to participate. I encourage everyone to comment with your answers to each assignment at the bottom of each post so that the group may benefit as a whole. If you are currently in the process of certification please inform your mentor that you have joined a study group and share the link with them- I do not want to leave anyone out of the loop. Archives
November 2017
COVD Certification Guide
|
