|
I am going to skip ahead a bit and start adding some content that has to do with the tools we use in the VT Room. I know that Multiple Choice Exams are coming up and want to make sure we focus the time where the test weighs the heaviest. We as therapists need to understand the tools we use in order to use them effectively with our patients. The pdf below of a PowerPoint is from a training I did with the staff at my office. I do not know what tools they will ask about or for that matter what questions will be asked on the MCE so I will attempt to post as many different tools as possible in the next week. Some may be original content like this one (though I will admit that I stole all the good bits from the masters of this field) and some may be links to sites that I found helpful when I was studying to take my MCE's. 
0 Comments
REFRACTIVE CONDITIONS: ASTIGMATISM Definition: Blurred vision due to an irregularity in the shape of the cornea or due to the shape of the lens inside the eye. Astigmatism is the result of an irregularly shaped cornea. There are two types of astigmatism, corneal and lenticular. When astigmatism is caused by an irregularity in the shape of the cornea, it is corneal astigmatism. When it is cause by an irregularity in the shape of the lens, it is called lenticular astigmatism. Corneal astigmatism is the most common. A normal eye has a rounded shape like a ball; however, an eye with astigmatism is shaped more like a football. Astigmatism can cause difficulty focusing at varying distances. Patients with myopia and hyperopia alike can have astigmatism. According to the AOA website “The specific cause of astigmatism is unknown. It can be hereditary and is usually present from birth. It can change as a child grows and may decrease or worsen over time.” Lenses are usually prescribed for the patient to help improve acuity. Vision therapy is not a cure for astigmatism, therefore, therapy is performed to help reduce or eliminate the need for prescription lenses. The first image below shows the difference in how the light enters a normal eye and an eye with astigmatism. The second image below shows the difference in the shapes of the cornea between a normal eye and an eye with astigmatism. 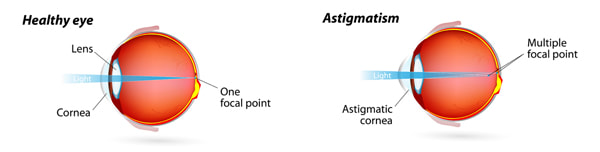 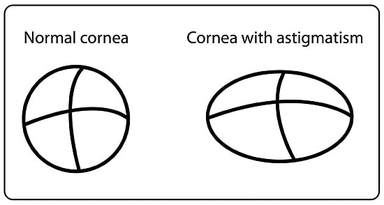 As with myopia and hyperopia, an eye with astigmatism doesn’t focus properly. Therefore, in therapy, activities that focus on improving flexibility of accommodation would be performed. Those activities would aid in shifting focus from near to far and vice versa more easily. In the process, the patient should see a reduction in the symptoms associated with astigmatism.
Symptoms of astigmatism:
Since examples of activities for myopia and hyperopia have already been discussed and we now know that a patient with either can have astigmatism, your assignment for this discussion is to share with the group an example of an activity that might be performed with a patient that has astigmatism. Please be as descriptive as possible for the benefit of the group. Also, discuss your definition of astigmatism and why you believe therapy is beneficial. I am going to post a bit out of order on this one while awaiting the next installment on Refractive Errors. This document was shared by the wonderful Linda Sanet, COVT with permission from COVD. This serves as an amazing glossary of terms that may be needed for future studying. Enjoy!
REFRACTIVE CONDITIONS: HYPEROPIA Definition: Inability to focus on objects at near – farsightedness Hyperopia, simply put, means the patient cannot focus on things up close. They are farsighted. This happens when the light entering the eye focuses behind the retina, as seen in the picture below. Unlike myopia in which there is too much curvature in the cornea, with hyperopia there is less curvature. This causes blur to happen at near distances. Having a large amount of blur can lead to strabismus or amblyopia as well. Many patients will need reading glasses or a bifocal in order to help them see things up close. A patient with hyperopia will have difficulty with up close work such as computer tasks or reading. The inability to focus properly can cause loss of place and reduced comprehension in what is being read. Hyperopia can be hereditary, can be a result of certain environmental factors, or can be a result of poor development. Vision therapy will not be a cure for hyperopia but will help the patient learn how to properly focus and may also have a reduction in prescription as a result of therapy. 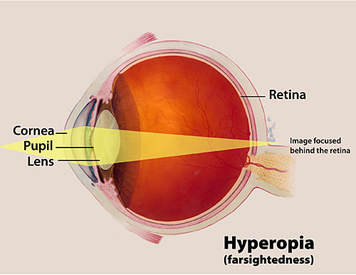 Symptoms of Hyperopia:
As with myopia, a patient with hyperopia struggles with flexibility of their accommodative system. In review, our accommodative abilities help with focusing from near to far and vice versa. Patients with hyperopia who have developed strabismus or amblyopia as a result, will also struggle with binocular dysfunction. These binocular dysfunctions will be discussed in detail at a later time. In therapy, one type of activity that would be performed would aid in strengthening accommodative abilities. One example of this type of activity would be Hart Chart Near Far Rock. Below you will find the instructions for this activity per OEPF. HART CHART NF (NEAR-FAR) ROCK PURPOSE: To provide the patient with the opportunity to have the necessary meaningful experience to shift the area in space from which the person will derive meaning from along the Z axis, expanding the range as well as the efficiency and accuracy of the shifts.
Please discuss your definition of hyperopia and its causes. Give an example of an activity that can be performed to help a patient with hyperopia. Please be as descriptive as possible for the benefit of the group. Also, feel free to share any resources you may have that you think would be helpful. This article is from the Journal of Behavioral Optometry and discusses the possibility that refractive errors may be the outcome of stress adaptive responses. Thought it might make a good addition to the otherwise often dry study of refractive errors. Click on the link below to go directly to the .pdf.  Hello everyone. I came across this study question sheet in some of my old documents and thought it would be good to share with the group. I am not sure of the source - it is quite old as it refers to COVTT instead of COVT which is the older acronym for therapist certification through COVD.
COVTT Study Guide Questions 1. Give an example of a vision therapy procedure that holds convergence constant and changes accommodation. 2. Give an example of a vision therapy technique that holds accommodation constant and changes convergence demands. 3. If a patient is having difficulty fusion the double window aperture rule what lens would help? 4. If a patient was having trouble doing the Eccentric Wall Circles, what lens would help? Why? 5. If a patient was wearing BO and was asked to quickly touch a bead on the Brock String, where would you predict his finger would land and why? If he did not, why not? 6. When a patient reports SOLI, what are some techniques to help him achieve SILO? 7. Patient has red lens over right eye, green over left. Target has red outline to right, green to left. Is this chiastopic (crossed) or orthopic (uncrossed) fusion? 8. If the patient is at 18 inches from the above target, would you add plus or minus to stress the system? Why? 9. Where would you expect her/him to locate the target? What size change from the original targets would they report if they had SILO? 10. Switch the filters on the above patient and repeat the question. 11.Bright lights and/or fluorescents will damage polarized slides and goggles? T or F 12. Colored filters and septums are dissociative instruments? T or F 13. A patient who reports seeing both the L and the R on the vectographic slides must be at the highest level of binocularity? T or F 14. Diplopia awareness techniques are appropriate in cases of AC? T or F 15. Describe the difference between MFBF and biocular activities. 16. What is a determining factor in anti-suppression techniques for an esotrope vs. an exotrope? 17. List three MFBF activities. 18. How do you know whether to put the red lens or green lens over the normally fixating eye during an anaglyphic procedure? 19. What is the key difference between simultaneous perception and superimposition? 20. Which testing procedure is the most unnatural in its visual demand? A. Vectograms B. Stereopscope C. Maddox Rod D. Bagolini (striated) lens 21. Which of the following are factors in utilizing anti-suppression training? A. Target movement B. Brightness C. Intermittent stimuli D. Target size E. All of the above F. A,B,D only 22. Which of the following is not a reliable tool in and of itself in monitoring suppression? A. “Beak” B. Binasal occluder C. Loose prism 23. Anaglyphic targets are an example of what degree of fusion? 24. How could you vary an Aperture Rule procedure so that you would efficiently be training in both base-out and base-in directions? 25. How can you check that your young, anxious to please patient is fusing when he says he is? 26. How can you help your patient perceive the fused targets location in space? 27. What might the therapist suggest to the patient if there is noticeable head movement when tracking a pursuit? 28. What might the therapist suggest to the patient who is trying to achieve SILO on the Vectogram? 29. Would amblyopia more likely be present in an esotrope or an exotrope? Why? 30.Define amblyopia and discuss its cause. 31. How does one test for amblyopia? 32. What are some types of amblyopia? 33. What are the symptoms? 34. Define Eccentric Fixation and describe techniques used in its treatment. 35. Define anisometropia. 36. What is the relationship of hand-eye activities to amblyopia? 37. Describe hand-eye activities used in the treatment of amblyopia and discuss how to increase or decrease the demand. 38. Discuss pleoptics, “tagging the macula” and the role of ocular motor accuracy in amblyopia. 39. Describe afterimage transfer and its use. When is it contraindicated? 40. Describe how the Haidinger Brush (MIT) is used in amblyopia training. 41. Describe the use of the TBI or ABE. 42. When is a PLUS lens prescribed in amblyopia? 43. Describe various MFBF activities their purpose and appropriate use. 44. In treating amblyopia with eccentric fixation eye-hand activities are seldom used? T or F 45. An infant with significant anisometropia, such that one eye is more hyperopic than the other is more likely to have amblyopia than if he was a myopic anisometrope. T or F 46. Eccentric fixation can be demonstrated with the Haidinger Brush. T or F 47. Describe the Hering-Bielschowsky test. How would eccentric fixation affect your findings? 48. How would you use the MIT to train NC? 49. What techniques would you use with a patient who is not aware of his body schema? 50. If a child holds fixation better when asked to touch, what does this tell the therapist about him? How would you move him to visual tracking free from tactile support? 51. Name some visual-tactile techniques. 52. How would you use parquetry blocks to teach form perception? 53. Give a home therapy technique to enhance form constancy. 54. How could the tachistoscope be used to teach visual closure? Hello everyone. Just a quick post to let you know that I am still here and working on content for future posts. If you have not done so already please peruse the most recent post on Myopia and post your answer to the assignment in the comments section below the post.
I wanted to remind you all that there are a great variety of study resources available on the internet now one of which is Quizlet where you can make your own flashcards good for studying for your MCE's or you can view sets of cards made by other people and shared publicly . I am posting a link below to card sets dealing with VT and encourage you to take a look through them to see if anything speaks to you. Enjoy! https://quizlet.com/subject/vision-therapy/ Hello to everyone still hanging in there with me! It has been a long and busy few months since I last posted. I embarked on this endeavor almost a year ago with all great intentions of making it the whole way through all of the topics on the Candidate Guide and it only took a few months before I could see what a gigantic task I was taking on alone. Life and work got in the way of my goal of creating a place to go for the answers you may be seeking in your certification journey.
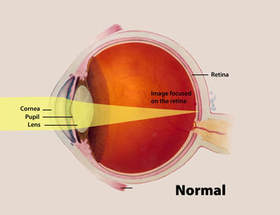
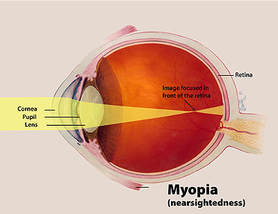
I am not one who is particularly good at asking for help but just the other day it occurred to me that in order to reach my goal here I was going to have to do exactly that. So I went onto the Vision Therapist's Forum and asked for help and guess what... I got it! Not that it is a big surprise since we as Vision Therapists are generally a group that love to help others. On that note I wanted to let you know to keep checking here in the upcoming weeks. I am so excited to share some amazing new posts from other therapists and a few from myself as well! Stay tuned... Michelle Beatty, COVT REFRACTIVE CONDITIONS: MYOPIA Definition: The inability to see things/focus far away; nearsightedness. When you hear the term myopia, it simply means that the patient with myopia is nearsighted. They can focus on things at near, but are unable to focus on things at a distance. Generally, myopia begins at a young age and progresses as the patient gets older. Myopia can also be inherited or can occur when a person does too much up close work such as reading or working on a computer. Myopia happens due to the curvature of the cornea being too much, and, as a result, the light that enters the eye is focused in front of the retina resulting in blur. Below is an image of light entering a normal eye and an image of light entering the eye of a person with myopia.
As mentioned before, a patient with myopia cannot focus on things at a distance. We want to improve their accommodative flexibility, meaning their ability to focus from near to far and from far to near without hindrance. Vision therapy will not be a cure for the patient; however, it is beneficial, in that, they may have a reduction in prescription and enhanced visual acuity, as well as, a new ability to accommodate properly so that they can focus better on targets farther away. Symptoms/Characteristics:
When working with a patient who has myopia, you want to improve their accommodative flexibility. As mentioned before, this means improving their ability to focus properly. One activity that can be done in office, as well as, at home is Brock String. Below are instructions for this activity per OEPF website. PURPOSE - To give immediate feedback to the patient as to whether both eyes are turned on, whether they are both pointed to the same place in space, and whether their perception of where a target is matches its real location. Also to let them become more familiar with how it feels to converge and diverge. The activity provides visual feedback to the patient as they attempt to move to various points of space and maintain proper centering and identification at each point. After practice in the office, this procedure is assigned for homework.
 (This activity can be loaded or unloaded as needed based upon the performance of the patient. Below is one way to load this activity per the OEPF website.)
BEAD JUMPING PURPOSE - To increase the ability to move from one point in space to another quickly and accurately and still maintain proper focus and depth perception. This activity uses visual feedback to allow the person to more quickly and accurately control the centering mechanism.
*Assignment*: Your assignment for this topic is to give your own description of myopia and how you would explain to a patient/parent that vision therapy can be beneficial. Also include an activity you would do with a patient who has myopia. Please be as descriptive as possible for the benefit of the group. Also, feel free to share any resources you may have that you think would be helpful. With the upcoming Annual Meeting and Oral Interviews I thought it would be a great time to share a fantastic article written by Robert Nurisio, COVT. You may find more of Robert's writing and wisdom on his blog accessible at https://vtworks.wordpress.com  I want to apologize for those in the group for my long absence from the group. A combination of the holidays, illness and training needs at the office where I work have kept me from updating for quite some time now.
For those who are in the certification process this year we will continue to work until the Annual Meeting in April. Though we may not be able to cover all topics before the MCE's this month we can still prep for Oral Interviews. I will do my best to update as frequently as I can as my hope is still to complete the topics on the Candidate Guide prior to the meeting. I may ask for some assistance from the group and if anyone is interested in taking on one of the topics and writing up some notes to prompt discussion I would be so appreciative as it seems there are not enough hours in the day. I hope everyone has been studying and please let me know if you have any questions or would like to pitch in and help out! Michelle Beatty, COVT Hello everyone since our next topic in the candidate guide is Refractive Conditions I am posting a link to an article by the AOA about Myopia. Though it does not list details on therapy for myopia it does give a very good definition and covers symptoms as well.  Hello everyone! I just wanted to say I am sorry it has been so quiet on here of late. I have just started training a new group of therapists and have been completely worn by the time I get home. I think I have hit my second wind so I am going to attempt to get back on track with the group. Later on today I should have next post/assignment posted but in the meantime I am attaching a link to a practice MCE that I created last year for folks I was mentoring. If the link does not work here for some reason you may find the same exam in the COVD Certification section accessible from the main page on the tab that says Practice MCE. Expect to hear more from me in the next few days, I know that for those taking the MCE in January that date is fast approaching and I want to help where I can. Practice MCE  As I mentioned in my most recent email to the group our next set of posts will deal with refractive conditions. I thought before we broach that subject it may be a good idea to make sure everyone has a basic grasp of the anatomy of the eye and how that effects vision. The video is brief (less than 10 minutes) but gives a really entertaining and detailed description of not only the parts of the eye but how they work and interact. Click on the pic below to watch...  Definition- Pursuits are slow movements which consist of the eye tracking a moving target. Linda Sanet, COVT describes them as "holding movements" whose purpose is to hold the object of regard still on the fovea. Due to the slower speed of a pursuit movement there is a certain amount of voluntary control where correction can be made during the movement unlike a saccade.  A quick and super goofy demonstration of smooth pursuits. Symptoms/Characteristics of a Pursuit Dysfunction-
Therapy- One of the great things I find about training accurate and efficient pursuits is that there is generally not a lot of equipment necessary. A patient can work on just watching his/her finger or I often use a penlight with a monster topper. Typically I will begin working laterally, then vertically once the patient is successful rotations such as circles and a smooth sideways figure eight. An example of this can be found in the video below using just a playing card as the target. Once the patient is smooth in all directions I begin asking questions (adding cognitive demand) which give me feedback as to how well developed the pursuit movement is. If it stops or pauses while the patient in answering the questions the movement is not yet well developed or automatic.
Below is an interesting article from the Journal of Vision - ARVO about eye movements and perception that may be worth a read...  Eye movements and perception: A selective review - ARVO JOV The assignment that goes along with this topic is as follows:
In the comments below please state your definition of pursuits, the signs and symptoms (your own list) when deficient and detailed instruction for one therapy activity you use to address difficulty with pursuit eye movements. Please be as descriptive as possible for the benefit of the group and if you have any links or resources to share please feel free to do so here. 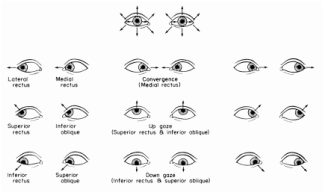 Today we will be discussing Saccadic Eye Movements. Again I have to tip my hat to Linda Sanet on this one because I love her description of Saccades as "Catching" movements. This to me is a great way to think about saccades, their purpose is to grasp a new object of regard by the fovea. Definition- Sudden voluntary change in fixation from one object of regard to another (definition via the Sanet Volumes). In addition to this sudden voluntary movement there is a certain type of “suppression” (for lack of a better term) or inhibition that takes place in order to avoid awareness of the visual smear during a saccade. :"Static visual stimuli are smeared across the retina during saccades, but in normal conditions this smear is not perceived. Instead, we perceive the visual scene as static and sharp. However, retinal smear is perceived if stimuli are shown only intrasaccadically, but not if the stimulus is additionally shown before a saccade begins, or after the saccade ends" (Campbell & Wurtz, 1978). As to exactly how the filtering process of that smear takes place is not known at this time though researchers think that it is inhibited at the LGN (Lateral Geniculate Body). In this section I also wanted to add a bit of information about the extraocular muscles since it is the firing of these muscles that drive saccadic movement.
For those of you who are interested in learning about the neurology behind eye movements below are links to a video from MIT Open Course Ware that deals with Neural Control of Visually Guided Eye Movements. The videos are lengthy and heavy but worth watching or bookmarking for future reference.  Below is another video about eye movements up close and in slow motion.  Symptoms/Signs when Deficient-
Therapy- In our office one activity we use early on in therapy to train saccadic accuracy is called Hart Chart Saccades and the procedure is as follows: Hart Chart Saccades Purpose: To improve the ability to organize and visually track while maintaining peripheral awareness. Materials: Letter Chart Technique: Level I – Straight Fixations 1.. The patient sits in a relaxed and balanced posture. 2. The Letter Chart is placed at eye level approximately 6’ away. 3. Instruct the patient to read the letters out loud in a rhythmic fashion without moving his head. The patient reads the entire chart proceeding in a left-to-right top-to- bottom fashion. Encourage the patient to maintain peripheral awareness of the whole chart and of other objects in the room. Level II – Line Interiors 1. Starting with the first line of letters, the patient reads out loud the 1st letter, then the last letter, then the 2nd letter, then the next-to-last letter, etc. Each line will be read from the ends to the middle in this fashion. 2. The patient is encouraged to maintain peripheral awareness of the whole chart and of other objects. Variations: 1. Use a metronome set to 60bpm 2..Add distractions such as saying other letters or repeating the alphabet. The assignment that goes along with this topic is as follows:
In the comments below please state your definition of saccades, the signs and symptoms (your own list) when deficient and detailed instruction for one therapy activity you use to address difficulty with saccadic eye movements. Please be as descriptive as possible for the benefit of the group and if you have any links or resources to share please feel free to do so here.  More Info on Microsaccades More Info on Microsaccades We are going to start slowly with one specific topic and break each one down individually. In this post we will be exploring Fixation. As far as a definition for Fixation my favorite (which I pulled in part from the Sanet Volumes) so far is: Definition- The act of directing the eye toward the object of regard causing, in the normal eye, the image of the object to be centered on the fovea. Fixations are a minute scanning motion not observable by the naked eye made up of high frequency tremors, slow drifts and micro saccades. These mini-movements serve to refresh the image on the retina. One of the main reasons I like this definition is because we often think of fixation as keeping the eyes completely still. This is not the case because if our eyes were completely still the image to which we are attending would disappear as it is not being refreshed on the retina. For anyone interested in more information about microsaccades at the right is a great website link (just click on the picture). An example of an optical illusion that is similar to this fading is called Troxler's Effect. To view this you fixate on the red dot for a few moments and you will see the peripheral blue halo disappear. It will reappear upon changing fixation.  I often think of fixation as being the underlying foundation for eye movements such as saccades and pursuits. If fixation is inadequate all other following eye movements will be inefficient and inaccurate. Since fixation is the foundation the signs/symptoms of deficient fixation would be much the same as with deficient pursuits/saccades Symptoms/Signs when Deficient-
Therapy- In our office one activity we use early on in therapy to train fixation awareness is called Peripheral Penny Snatch and the activity goes as follows; Peripheral Penny Snatch Purpose: To help the patient improve ability to hold their eyes still while maintaining peripheral awareness. Materials: Pennies, plastic cups Technique: 1. Sit on floor facing patient and put a plastic cup in front of you. 2. Instruct patient to sit facing you, keep their eyes on your eyes and don’t look away. 3. Take a penny in each hand and pinch between your index finger and thumb holding them just past your shoulders to start. 4. Ask the patient to take the pennies from your fingertips without looking away from your eyes. Once the patient has successfully taken the penny from the assistant’s fingertip he/she puts it into the cup while maintaining eye contact. If unsuccessful the patient tries again. 5. Give patient feedback appropriate to performance. For example: “Good, you kept your eyes on mine for a little while, and then you peeked. Let’s try it again…” 6. Repeat while holding the penny at a different starting point each time. 7. Since self-awareness is a goal of vision therapy, when possible, ask patient, “How did you do that time?”, etc. Aspects to be emphasized: 1. Awareness of maintaining eye contact (Did they peek?) and peripheral vision. 2. Patient should have good posture, blink and breathe normally. 3. Patient’s ability to grab pennies accurately. The assignment that goes along with this topic is as follows: Hello and welcome to our online study group. This group will be available to any therapist who is currently in the process or will soon be in the process of certifying through COVD. Please follow the directions on the right hand page to join in.
My current plan for the group is to follow the flow of the COVT Candidate Guide. I will post relevant information/articles/book excerpts in these blog type posts. Any questions, answers or comments may be made in the comment section below each post. I will contact anyone who has asked to be included via email when the first post goes up so please email me if you wish to join in, Michelle Beatty, COVT |
VT Study GroupThis group is public and open to anyone that would like to participate. I encourage everyone to comment with your answers to each assignment at the bottom of each post so that the group may benefit as a whole. If you are currently in the process of certification please inform your mentor that you have joined a study group and share the link with them- I do not want to leave anyone out of the loop. Archives
November 2017
COVD Certification Guide
|
|||||||